Brachial Plexus Birth Palsy (BPBP), often referred to as Erb’s Palsy, is a condition involving injury to the network of nerves (the brachial plexus) that controls movement and sensation in the shoulder, arm and hand.
1. Overview & Causes
- Definition: A flaccid paralysis or weakness of the upper limb caused by a traction (stretching) injury to the brachial plexus during birth.
- Incidence: Occurs in approximately 1 to 4 per 1,000 live births.
- Mechanism: Typically happens during a difficult delivery when the infant’s neck is stretched to the side (often associated with shoulder dystocia, where the shoulder becomes stuck behind the mother's pelvic bone).
- Risk Factors: High birth weight (macrosomia), maternal diabetes, prolonged labor and breech delivery. However, it can occur in babies with no risk factors and even during C-sections.
2. Types of Injury
The severity depends on the type of nerve damage:
- Neurapraxia: A stretch that "shocks" the nerve but does not tear it. This is the most common and usually heals within 3 months.
- Neuroma: A stretch that damages some fibers, leading to scar tissue that may press on healthy nerves. Partial recovery is common.
- Rupture: The nerve itself is torn and cannot heal on its own; it requires surgical repair.
- Avulsion: The nerve is torn away from the spinal cord. This is the most severe form and cannot be repaired directly; it usually requires nerve transfers.
3. Common Presentations
- Erb’s Palsy (C5-C6): Most common. The arm hangs at the side, rotated inward, with the forearm pronated and wrist flexed (the "Waiter’s Tip" position). The child cannot move the shoulder or bend the elbow but may move their fingers.
- Klumpke’s Palsy (C8-T1): Affects the lower nerves, primarily impacting the hand and wrist. This can result in a "claw hand" appearance.
- Total Plexus Palsy (C5-T1): The entire arm and hand are affected, resulting in complete paralysis and loss of feeling.
4. Diagnosis & Evaluation
- Clinical Exam: Diagnosis is primarily made through physical examination at birth, looking for a lack of spontaneous movement or an absent Moro reflex (startle reflex) on the affected side.
- Monitoring: Doctors monitor the "return of the biceps" (elbow flexion). If the child can bend their elbow against gravity by 3 months, the prognosis for full recovery is very high.
- Imaging: X-rays may be used to rule out fractures (clavicle or humerus). MRI or ultrasound may be used later to check for shoulder joint dislocation (glenohumeral dysplasia).
5. Treatment & Management
- Therapy (Primary Treatment): Daily physical and occupational therapy are essential. Exercises focus on maintaining range of motion (ROM) to prevent "contractures" (permanent stiffening of the joints).
- Botox: In some cases, Botox is injected into stronger "competing" muscles to allow weaker nerves a chance to function and to prevent joint deformities.
- Nerve Surgery: If there is no significant recovery (specifically of the biceps) by 3–9 months, microsurgery (nerve grafts or transfers) may be recommended.
- Secondary Surgery: For older children with residual weakness, surgeons may perform tendon transfers (moving a working muscle to do the job of a paralyzed one) or osteotomies (realigning bones) to improve function.
6. Prognosis
- High Recovery Rate: The majority of infants (roughly 80–90%) will recover nearly normal function within the first 3 to 12 months.
- Long-term: Children who do not show signs of recovery by 3 months are at a higher risk for permanent deficits and may require lifelong monitoring to manage bone growth and joint health.
Cases - Videos
Case - 1
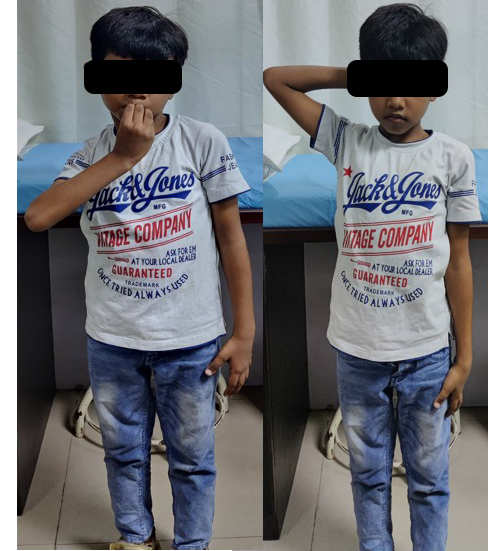
Before

Pre-operative clinical images showing limitation of hand to neck movements and trumpeting of more than 90 degrees
After

Same child one year after surgery showing good and comfortable hand to neck movements and trumpeting less than 40 degrees.
Case - 2
MISR & TT
Before

Pre-operative clinical images showing limitation of hand to neck movements and trumpeting of more than 90 degrees
After