In paediatric orthopaedics, the phrase "Children are not just small adults" is most evident in fracture care. Because children's bones are still developing, they have unique anatomical features—like growth plates and a thicker "skin" around the bone (periosteum)—that change how they break and how they heal.
1. Why Paediatric Fractures Are Different
- Growth Plates (Physis): Children have areas of developing cartilage at the ends of long bones. These are the "weak links" in the skeleton and are more likely to fracture than the tough ligaments surrounding them.
- Thick Periosteum: The connective tissue covering the bone is much thicker in children. It helps stabilize fractures and provides a rich blood supply, leading to faster healing (weeks instead of months).
- Flexibility: Paediatric bones are more "porous" and less dense than adult bones. They can often bend or buckle without snapping completely.
- Remodeling: Because children are still growing, their bodies have a remarkable ability to "straighten out" a bone that healed slightly crooked over time.
2. Unique Types of Paediatric Fractures
Because their bones are pliable, children experience fracture patterns rarely seen in adults:
- Buckle (Torus) Fracture: The most common paediatric fracture. One side of the bone "buckles" or bulges outward due to compression (often from a fall on an outstretched hand). These are stable and usually heal in a simple splint or cast.
- Greenstick Fracture: Similar to a young green branch, the bone breaks on one side but only bends on the other.
- Plastic Deformation: The bone bows or curves significantly under pressure but does not show a visible "crack" on an X-ray.
- Growth Plate (Physeal) Fracture: A break that crosses the growth plate. These are classified using the Salter-Harris system (Types I through V). Accurate alignment is crucial here to prevent the limb from growing crookedly or stopping growth early.
3. Common Fracture Locations
Location
- Forearm/Wrist: Account for up to 50% of all childhood fractures. Usually caused by falling onto an outstretched arm (FOOSH).
- Elbow: Often "Supracondylar" fractures. These are serious because they occur near major nerves and blood vessels; they frequently require surgery with pins.
- Clavicle (Collarbone): Very common in active children and newborns; almost always treated with a simple sling.
- Toddler’s Fracture: A faint, spiral fracture of the tibia (shin bone) in young children who are just learning to walk. It can be hard to see on X-rays.
4. Treatment Approaches
Most paediatric fractures can be treated without surgery because of the bone's ability to remodel.
- Observation/Splinting: For stable "buckle" fractures.
- Closed Reduction: The doctor "sets" the bone by manually moving it into place while the child is sedated, followed by a cast.
- Open Reduction & Internal Fixation (Surgery): Used for unstable fractures, fractures that enter a joint, or severe growth plate injuries. Small pins, wires, or screws are often used to hold the bone while it heals.
5. Complications to Watch For
- Growth Arrest: If a growth plate is damaged, one limb may end up shorter than the other.
- Angular Deformity: The bone may grow at an angle (e.g., "knock-knees" or "bow-legs").
- Nerve/Vessel Injury: Especially common in elbow fractures. Parents should watch for "the 5 Ps": Pain (uncontrolled), Pallor (pale skin), Pulselessness, Paresthesia (numbness) and Paralysis.
Case - Video
Case - 1
Elbow Fracture
Before
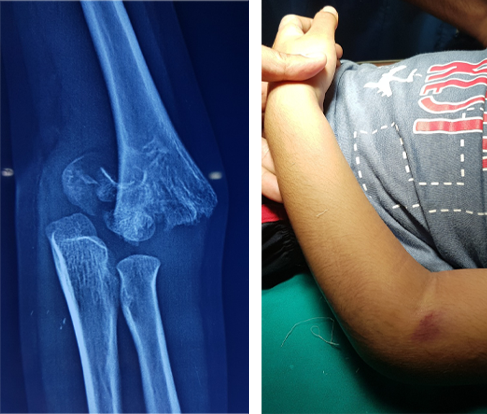
Swelling, Pain, Bruises and inability to move the elbow
After
Treatment may vary from as simple as sling application to an urgent surgery depending upon the severity of fracture
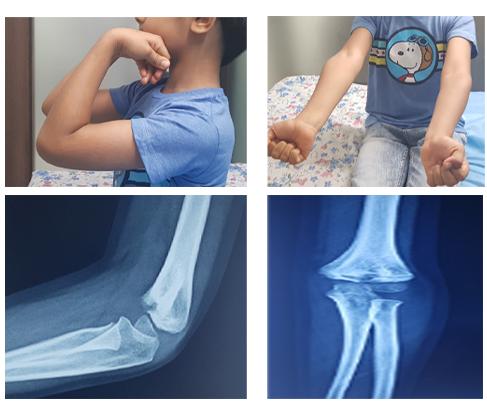
Case - 2
Supracondylar humerus fractures in Kids
Before
Pre Operative Lateral & AP view of Left elbow
After

2 month Post Operative AP and Lateral view of the left elbow
After

Full extension & full flexion of both the elbows
Case - 3
Fractures due to birth trauma
Before
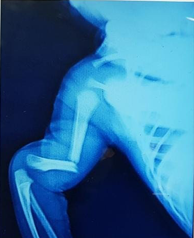
Humerus shaft fracture at birth
After

Managed conservatively with vulpeau's sling
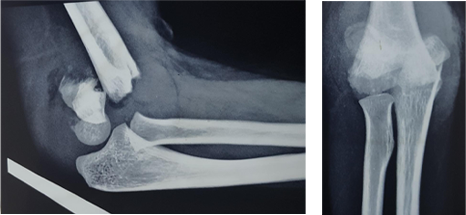
Case - 4
Close reduction of displaced finger fracture in a 6 year old girl
Before

Ap & Oblique X rays
showing fracture and
displacement at base of left little finger
Post reduction images
showing complete correction of the
deformity
After
